Parkinson’s disease is progressive, debilitating, and — when it prevents you from working — should qualify you for long-term disability (LTD) benefits. Yet many Ontarians with Parkinson’s find their claims delayed, underpaid, or outright denied. The reason is rarely the diagnosis itself. It is almost always the medical evidence.
Insurance companies require far more than a doctor’s letter confirming the diagnosis. They want objective, measurable, regularly updated documentation of how your symptoms impair your ability to work — both now and over time. For a condition like Parkinson’s, whose symptoms fluctuate hour by hour and worsen unpredictably, that evidentiary standard can feel impossibly high. Understanding exactly what insurers look for — and where the gaps appear — is the first step toward protecting your benefits.
This guide focuses specifically on the medical evidence, documentation strategy, and insurer tactics that matter most to Parkinson’s LTD claimants in Canada. If you are wondering more broadly whether you qualify for LTD, our colleagues have addressed that in our general long-term disability practice resource. This article goes deeper: into the specialist reports, objective tests, cognitive assessments, IME pitfalls, and appeal strategies that are unique to a Parkinson’s claim.

Table of Contents
- What Medical Evidence Do Insurers Require to Approve Parkinson’s Disease LTD Claims?
- Why Do Insurers Deny Parkinson’s LTD Claims at the ‘Own Occupation’ Stage?
- What Objective Tests and Biomarkers Prove Parkinson’s Severity for LTD Approval?
- How Do IME Physicians Underestimate Parkinson’s Cognitive Decline and Motor Deterioration?
- What Happens to Parkinson’s Claimants at the 24-Month ‘Any Occupation’ Definition Switch?
- How Do You Appeal a Denied Parkinson’s LTD Claim With Medical Evidence?
- Building a Long-Term Documentation Strategy for Progressive Parkinson’s
What Medical Evidence Do Insurers Require to Approve Parkinson’s Disease LTD Claims?
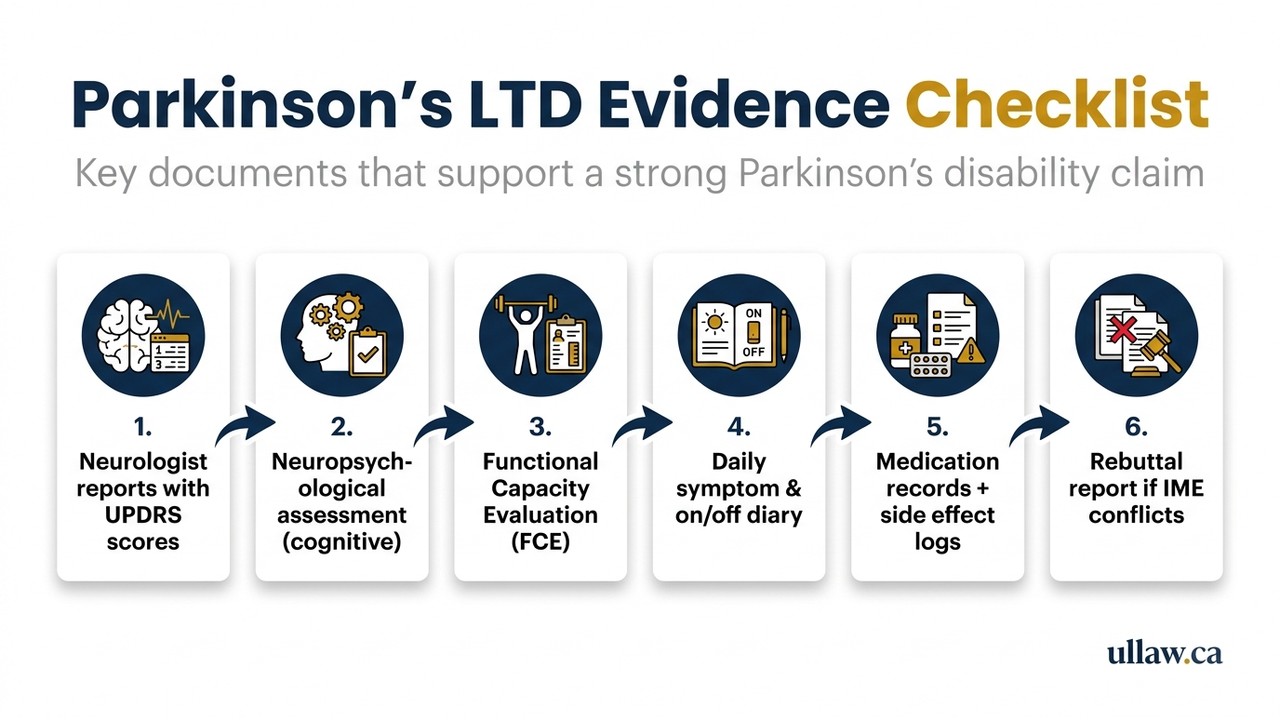
Insurance companies in Canada assess LTD claims under the terms of your specific group or individual policy, but the evidentiary demands follow a recognisable pattern. For Parkinson’s disease, a successful initial claim file typically includes all of the following.
Neurologist’s Clinical Reports
A diagnosis and ongoing care from a movement disorder neurologist — ideally a subspecialist — carries the most weight. Generic family physician notes alone are rarely sufficient. The neurologist’s reports should document:
- Confirmed diagnosis (and, where relevant, which subtype — e.g., tremor-dominant vs. postural instability/gait difficulty)
- Hoehn & Yahr scale staging at each visit
- Response (or lack thereof) to levodopa and other medications
- Frequency and severity of “off” periods when medication wears off
- Any dyskinesias caused by long-term medication use
Functional Capacity Evidence
Diagnosis alone does not satisfy an insurer. They want to know what you cannot do. A Functional Capacity Evaluation (FCE) conducted by an occupational therapist measures your physical tolerances — sitting, standing, walking, fine motor tasks, lifting. For Parkinson’s, FCEs must be interpreted carefully because performance often varies significantly with the time of day and medication cycle.
Attending Physician’s Statement (APS)
Your insurer will send an Attending Physician’s Statement form. This must be completed — ideally by your neurologist, not just your GP — with specificity about restrictions and limitations. Vague answers like “patient is unable to work” without functional detail give adjusters reasons to request more information or deny the claim.
Cognitive and Neuropsychological Assessments
Parkinson’s frequently causes Parkinson’s disease dementia (PDD) or mild cognitive impairment (MCI). If cognitive symptoms are part of your picture — and they often are, even early on — a formal neuropsychological assessment documenting deficits in executive function, processing speed, memory, and attention is critical.
Medication Records and Side Effect Documentation
Treatment records showing your medication regimen, dosage adjustments, and documented side effects (fatigue, cognitive fog, impulse control issues, orthostatic hypotension) all help demonstrate the full functional impact of the disease.
Other Specialist Reports
Depending on your presentation, supportive reports from a physiotherapist, speech-language pathologist, or psychiatrist (for depression and anxiety, which are extremely common in Parkinson’s) may round out a complete file.
You can review the relevant insurance regulatory framework through the Ontario Insurance Act and related legislation, which governs most group benefit policies in the province.
Why Do Insurers Deny Parkinson’s LTD Claims at the ‘Own Occupation’ Stage?
The first definition period in most LTD policies — typically the first 24 months of benefit — requires only that you be unable to perform the essential duties of your own occupation. You would think a Parkinson’s diagnosis would make this straightforward. It rarely is.
“You Can Still Do a Sedentary Job”
Insurers frequently argue that because your role sounds desk-based, your tremors, rigidity, and fatigue do not actually stop you from working. They ignore the cognitive demands, the embarrassment of visible symptoms in a professional setting, the unpredictability of “off” periods, and the exhaustion that often follows a few hours of even minimal activity.
Incomplete or Vague Medical Evidence
If your APS form is filled out by a busy GP with generic answers, or if your neurologist’s notes do not describe functional impairment in job-specific terms, the adjuster will use those gaps against you. An insurer’s job is to look for reasons to say no.
Selective Reading of Medical Records
Adjusters are trained to highlight the good days documented in clinical notes — “patient reports improvement with new medication dose” — while glossing over the broader pattern of deterioration. Parkinson’s symptoms fluctuate; a single positive clinic note does not mean you are able to sustain full-time work.
Surveillance
Short-term video surveillance of a claimant walking to a car or grocery shopping is sometimes used to suggest functionality. Surveillance almost never captures an “off” period, a freezing episode, or the exhaustion that follows even brief exertion.
What You Can Do
Your neurologist’s reports should explicitly address work-specific functional limitations, not just clinical markers. Your file should include a personal pain and symptom diary — a daily log documenting “on” vs. “off” periods, freezing episodes, fall risk, fatigue levels, and cognitive fluctuations. This contemporaneous evidence is difficult for insurers to dismiss.
If your claim has already been denied at this stage, our long-term disability legal team can review your file and identify the evidentiary gaps.
What Objective Tests and Biomarkers Prove Parkinson’s Severity for LTD Approval?
Insurers and their medical reviewers respect objective data. While Parkinson’s has historically been a clinical diagnosis with no single definitive biomarker, a growing toolkit of objective assessments can substantiate the severity of your condition.
Movement and Motor Assessments
- MDS-UPDRS (Movement Disorder Society Unified Parkinson’s Disease Rating Scale): The gold standard rating tool for Parkinson’s motor and non-motor symptoms. Serial UPDRS scores over time showing progression are compelling longitudinal evidence.
- Timed Up and Go (TUG) test: A simple but objective mobility measure documented in physiotherapy or neurology notes.
- Gait analysis: Formal computerised gait analysis can quantify freezing of gait, stride length, and balance impairment — deficits that are impossible to fake and directly map to workplace limitations.
- Tremor quantification: Accelerometry-based tremor measurement provides objective data beyond subjective clinical observation.
Imaging
- DaTscan (Ioflupane SPECT imaging): Approved in Canada, a DaTscan demonstrates dopaminergic deficiency in the striatum. While it does not measure severity, it can help confirm diagnosis and counter any insurer suggestion that your symptoms have another, less disabling cause.
- Brain MRI: While MRI cannot diagnose Parkinson’s, it can rule out other causes and, in some cases, show relevant structural findings.
Neuropsychological Testing
For cognitive impairment, standardised tools including the Montreal Cognitive Assessment (MoCA), Trail Making Test, and a full neuropsychological battery provide quantitative evidence of executive dysfunction and processing speed deficits — symptoms that directly impair safety and productivity at work.
Sleep Studies
REM sleep behaviour disorder (RBD) is strongly associated with Parkinson’s and is highly disabling. A formal polysomnography documenting RBD, as well as excessive daytime sleepiness scores (Epworth Sleepiness Scale), can support claims of fatigue-related work impairment.
Autonomic Testing
Parkinson’s frequently causes orthostatic hypotension (dangerous blood pressure drops on standing), bladder dysfunction, and other autonomic features. Documented tilt table testing or autonomic function studies add to the picture.
The Canadian Neurological Sciences Federation and neurological subspecialty bodies publish clinical guidelines that can support the validity and relevance of these assessments in your claim file.
How Do IME Physicians Underestimate Parkinson’s Cognitive Decline and Motor Deterioration?
An Independent Medical Examination (IME) is rarely truly independent. The insurer selects, retains, and pays the examining physician — a structural conflict of interest that frequently produces reports that minimise your limitations.
The Single-Snapshot Problem
Parkinson’s symptoms fluctuate dramatically. An IME is a one-to-three-hour snapshot. If you happen to be in an “on” period when medication is working well, you may walk steadily and answer questions clearly. The IME physician may document this as your baseline — when it is not.
What to do: Ask your neurologist to write a letter specifically explaining the “on-off” phenomenon and how a brief examination cannot reliably capture your functional baseline. Bring your symptom diary to the IME.
Cognitive Testing is Often Inadequate
Many IME physicians are not neuropsychologists. They may administer a brief screening tool (such as the MoCA) and, if you score within normal limits on that single test, conclude that cognitive impairment is not a significant issue. This misses subtle executive dysfunction — difficulty with planning, multitasking, working memory, and processing speed — that may be devastating to your ability to perform your job even when the MoCA score appears acceptable.
What to do: Ensure your file contains a full neuropsychological assessment from a qualified neuropsychologist before the IME. The IME physician then cannot create the evidentiary record from scratch.
Dismissing Non-Motor Symptoms
Fatigue, depression, anxiety, apathy, pain, and autonomic dysfunction are often minimised in IME reports because they are less visible than tremor or rigidity. IME physicians may note them briefly and then conclude — without analysis — that they are manageable.
Failure to Review the Full Record
IME physicians sometimes review only selected records provided by the insurer. You have the right to know what records were provided and, through your legal counsel, to challenge an opinion based on an incomplete review.
Your Rights Regarding IMEs
You are generally entitled to have a support person present and to receive a copy of the IME report. If the report contains factual errors or ignores key clinical evidence, your own treating specialists can provide rebuttal reports — these are powerful tools in an appeal.
For more on the LTD appeal process generally, see our resource on what to do when LTD is denied.
What Happens to Parkinson’s Claimants at the 24-Month ‘Any Occupation’ Definition Switch?
The 24-month definition change is one of the most dangerous moments in any LTD claim — and it is especially fraught for people with Parkinson’s disease.
What the Definition Switch Means
Most group LTD policies pay benefits for the first 24 months if you cannot perform your own occupation. After that, the policy typically switches to a stricter standard: you must be unable to perform any occupation for which you are reasonably suited by education, training, or experience. This is sometimes called the “any occ” definition.
Why This Hits Parkinson’s Claimants Hard
Insurers routinely argue at the 24-month mark that a Parkinson’s patient who was, say, a senior manager or a skilled tradesperson is now capable of performing a sedentary, lower-demand role — perhaps a telephone receptionist or a data entry clerk. The insurer may commission a vocational assessment identifying these theoretical jobs and use it to terminate benefits.
This ignores the reality that Parkinson’s is progressive. At 24 months, many patients are significantly more impaired than they were at onset. Cognitive symptoms, postural instability, fall risk, medication side effects, and fatigue often make even simple sedentary roles unsustainable.
What Evidence Matters at the 24-Month Mark
- Updated neurologist report specifically addressing whether you can sustain competitive employment in any capacity, full-time, reliably, and safely
- Updated neuropsychological assessment — cognitive decline typically progresses and an older assessment may understate your current impairment
- Updated FCE — functional capacity often declines; a new evaluation closer to the definition change gives your claim a current, objective foundation
- Vocational rebuttal evidence — if the insurer identifies “suitable” jobs, your lawyer can retain a vocational expert to challenge whether those roles are genuinely feasible for someone with your specific Parkinson’s profile
Preparing in Advance
Do not wait until your benefits are terminated to update your medical file. Ideally, begin collecting updated documentation three to six months before the 24-month mark so there is no gap in your evidentiary record.
The Ontario e-Laws database contains the Insurance Act and its regulations, which set out some of the procedural rights that apply to Ontario policyholders throughout the claim lifecycle.
How Do You Appeal a Denied Parkinson’s LTD Claim With Medical Evidence?
A denied claim is not the end of the road. Most LTD policies provide an internal appeal process, and Ontario claimants also have the option of pursuing a civil lawsuit against the insurer. Either path requires a strategically built medical record.
Step 1: Get the Denial Letter and Understand the Reason
Insurers are required to explain why they denied or terminated your claim. Read the letter carefully. Common stated reasons include: insufficient medical evidence of total disability; your condition does not prevent any gainful employment; a peer review physician does not agree with your treating doctor’s opinion.
Step 2: Request Your Full Claim File
You are entitled to request all documents in your claims file, including peer review reports, IME reports, surveillance notes, and the records the insurer reviewed. This is critical — you cannot challenge what you cannot see.
Step 3: Build the Evidentiary Gaps
Compare what the insurer relied on against your actual medical picture. Common gaps to address:
- No specialist report → Obtain a detailed report from your movement disorder neurologist addressing the insurer’s specific stated concerns
- Outdated assessments → Commission a fresh neuropsychological evaluation and FCE
- IME contradicts treating specialist → Retain your neurologist or an independent neurological expert to write a rebuttal report addressing the IME findings point by point
- Missing symptom documentation → Submit your symptom diary and sworn statements from family members describing the daily reality of your functioning
Step 4: Internal Appeal
Submit a written appeal with all supplementary evidence. Set out clearly, in plain language, why each of the insurer’s stated reasons is contradicted by the evidence. Insist on a fresh review by someone not involved in the original decision.
Step 5: Legal Action
If the internal appeal fails — or if your policy does not provide a meaningful appeal mechanism — you may have the right to bring a civil claim against the insurer in Ontario court. Time limits apply. Under the Ontario Insurance Act, and depending on your policy terms, there are strict limitation periods for commencing legal action after a denial. Do not delay.
Why a Lawyer Matters at the Appeal Stage
Insurers have experienced claims teams and medical reviewers. A plaintiff-side disability lawyer understands the evidentiary standards, knows which experts carry weight, and can negotiate or litigate from a position of preparation. Explore your options with our long-term disability legal team before limitation deadlines pass.
For context on how Canadian courts and tribunals approach disability claims, CanLII provides free access to relevant Ontario and federal case law that your lawyer can use to anchor your appeal.
Building a Long-Term Documentation Strategy for Progressive Parkinson’s
Because Parkinson’s is a progressive condition, your medical evidence must grow and evolve alongside your symptoms. A claim file that was strong at onset may be dangerously thin two or three years later if it has not been updated. Here is how to maintain a living record.
See Your Neurologist Regularly — and Document Every Visit
Aim for neurologist appointments at least every three to six months. Each visit should generate a clinical note that includes updated UPDRS scoring, a description of current medication and any adjustments, and specific comments on functional change since the last visit. Ask your neurologist to note your functional limitations — not just your clinical status.
Keep a Symptom Diary
A daily log — even simple notes on your phone — documenting “on” and “off” periods, freezing episodes, falls or near-falls, cognitive difficulties, mood, sleep quality, and energy levels creates an unbroken record that is very difficult for an insurer to dismiss. If you have a caregiver or family member, their observations are equally valuable.
Photograph and Video Evidence
With appropriate care around privacy, brief videos recorded by a family member during “off” periods or freezing episodes can be powerful evidence — a direct counter to surveillance footage taken on a good day.
Coordinate Your Care Team
Ensure your GP, neurologist, physiotherapist, occupational therapist, neuropsychologist, and any mental health providers are communicating. A fragmented file with inconsistent observations gives adjusters room to doubt. A coordinated, consistent narrative across providers is much harder to undermine.
Understand Your Policy’s Reporting Obligations
Most LTD policies require you to provide updated medical information on a schedule. Missing a required update can be used to suspend or terminate benefits. Know your deadlines, and ensure your physicians are responsive to your insurer’s forms and requests.
Talk to a UL Lawyers Team Member
If your Parkinson’s disease LTD claim has been denied, delayed, or is approaching the 24-month definition change, you do not have to navigate the insurer’s process alone. Contact our long-term disability team for a free, no-obligation consultation. We work on a contingency basis for LTD matters, meaning you pay nothing unless we recover benefits for you. Let us review your file and tell you honestly where you stand.